
What Is Peripheral Artery Disease (PAD)?
A Complete Guide to Symptoms, Diagnosis & Treatment
A patient-friendly guide by RealMedVision
Last Update – May 2026
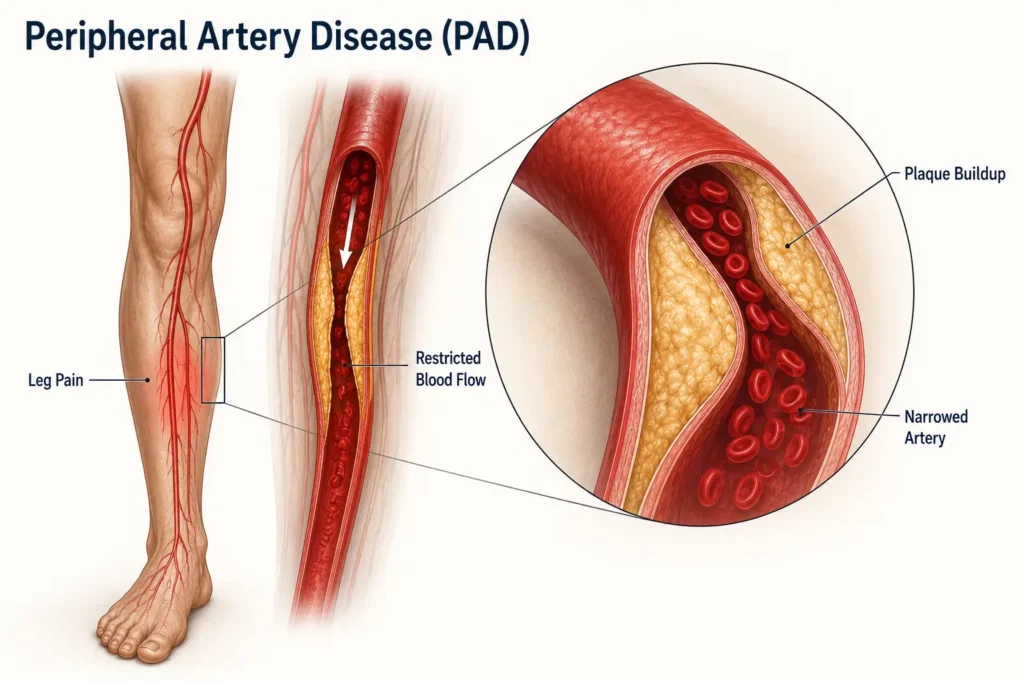
Peripheral Artery Disease (PAD) is a circulation problem in which narrowed arteries reduce blood flow to the legs and feet. It is usually caused by fatty plaque buildup inside the arteries, known as atherosclerosis. Common symptoms include leg pain while walking, cold feet, numbness, muscle cramps, and slow-healing wounds. If left untreated, PAD can increase the risk of heart attack, stroke, and serious circulation problems.
Early Symptoms of Peripheral Artery Disease
- Leg pain while walking (intermittent claudication)
- Cold feet or toes
- Muscle cramps in the calves
- Numbness or heaviness in the legs
- Slow-healing wounds on the feet
- Weak leg pulses
- Skin color changes in the legs
Silent Symptoms of Peripheral Artery Disease
Some people with Peripheral Artery Disease (PAD), especially diabetic patients, may never notice obvious leg pain in the early stages. Instead, the disease may develop silently with mild symptoms such as:
- Leg tiredness or heaviness
- Cold toes or cold feet
- Mild numbness in the legs
- Reduced walking stamina
- Slow nail growth
- Foot wounds that heal slowly
- Skin color changes in the feet or legs
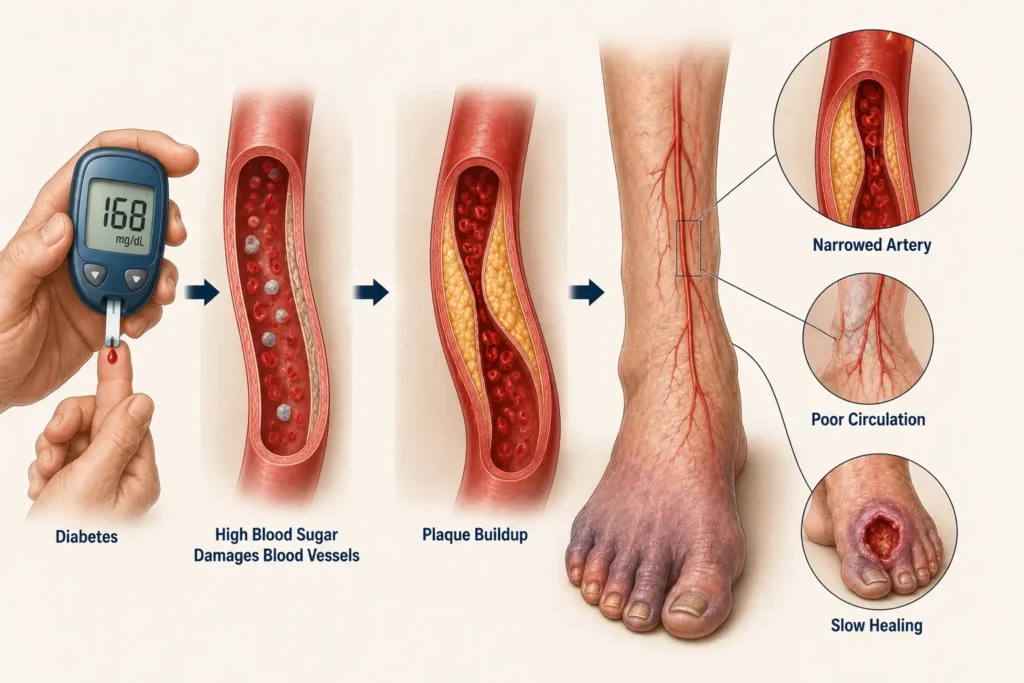
In diabetic patients, nerve damage known as diabetic neuropathy can reduce pain sensation, making PAD much harder to detect early. This is why people with diabetes should pay close attention to even small changes in their feet and legs, especially if they smoke or have high blood pressure or high cholesterol.
Is Peripheral Artery Disease Dangerous?
Yes. Peripheral Artery Disease (PAD) can become serious when blood flow to the legs becomes severely reduced. It may lead to severe leg pain, infections, slow-healing wounds, and in advanced cases, tissue damage or limb-threatening complications.
What makes PAD even more concerning is that it is not only a leg circulation problem. Doctors consider it a warning sign of artery disease throughout the body. People with PAD have a much higher risk of heart attack and stroke — especially smokers, diabetic patients, and those with high blood pressure or high cholesterol.
This article is my attempt to explain PAD the way I would explain it to a patient sitting in front of me. No unnecessary jargon. No complicated diagrams. Just clear, honest information that you can actually use.
What You Will Learn
By the end of this guide, you will understand:
- How PAD develops inside the arteries
- Early warning signs and silent symptoms
- Main causes and risk factors
- Why PAD is dangerous for diabetics and smokers
- The difference between PAD pain and normal leg cramps
- How poor circulation affects the legs and feet
- When leg pain may become serious
- How doctors diagnose PAD using the ABI test
- Medicines and treatment options for PAD
- When surgery or angioplasty may be needed
- Lifestyle changes that improve blood circulation
- What happens if PAD is left untreated
- How PAD increases heart attack and stroke risk
- When to see a doctor immediately
Global Epidemiology and Mortality
Let me give you a sense of how widespread this disease really is.
According to the Global Burden of Disease Study published in 2019, more than 230 million people across the world are currently living with Peripheral Artery Disease. That is more than the entire population of Brazil. And these are only the diagnosed cases. Millions more are walking around with narrowed leg arteries and no idea.
The disease does not affect everyone equally. Prevalence rises sharply after the age of 50, and the burden is heaviest in regions like South Asia, Sub-Saharan Africa, and Eastern Europe — areas where access to early screening and cardiovascular care is often limited. These trends have made peripheral artery disease symptoms an increasingly important public health concern worldwide.
In India specifically, data discussed in cardiology consensus meetings in 2023 has shown a worrying increase in PAD cases — particularly among urban populations with diabetes. The combination of rapidly changing lifestyles, high rates of smoking, and poorly controlled blood sugar is creating a perfect storm.
Now here is what really concerns me about PAD from a mortality perspective. Most patients do not die from their leg disease. They die from heart attacks and strokes. A major study published in JAMA Cardiology in 2017 showed that patients with PAD carry a two to three times higher risk of having a heart attack or stroke compared to those without the disease.
The World Health Organization has long emphasized that atherosclerotic diseases are the leading cause of non-communicable disease deaths worldwide.
This is why we take Peripheral Artery Disease (PAD) seriously—not just for the leg, but for the whole body.
Scientific Foundations: Who Shaped Our Understanding?
Medicine is built on the shoulders of researchers who asked the right questions at the right time. Understanding PAD symptoms and vascular disease as we know them today would not be possible without a few key figures.
Dr. Peter Libby
At Harvard Medical School, through his work in the 1990s, he fundamentally changed how we think about peripheral artery disease and arterial disease. He established that atherosclerosis is not just fat accumulation—it is an inflammatory process. The body’s own immune system is involved in building those plaques inside arteries. This insight changed treatment strategies for PAD and cardiovascular disease globally.
Dr. Valentin Fuster
At Mount Sinai, he contributed extensively to understanding why plaques rupture — which is what triggers sudden heart attacks and strokes. His work in the early 2000s helped explain why some patients with Peripheral Artery Disease (PAD) develop sudden vascular events even before they develop severe limb symptoms or noticeable Peripheral Artery Disease symptoms.
Dr. Mark Creager
At Dartmouth, through his contributions to the 2012 American College of Cardiology statements, he helped firmly establish Peripheral Artery Disease as a systemic vascular disease rather than just a peripheral limb problem. He pushed the cardiology community to treat Peripheral Artery Disease symptoms with the same seriousness as coronary artery disease.
Dr. Alan Hirsch
at the University of Minnesota developed much of the diagnostic framework we use today. His 2001 work helped define the clinical criteria and screening protocols that are now standard practice.
Dr. Gregory Roth
at the University of Washington led the Global Burden of Disease 2019 estimates, giving the world its most comprehensive picture of how many people PAD truly affects.
Large-scale research from Johns Hopkins University, the University of Oxford, Harvard, Cambridge, and ETH Zurich has continued to advance our understanding of vascular biology, endothelial function, and plaque behavior—forming the backbone of modern PAD management.
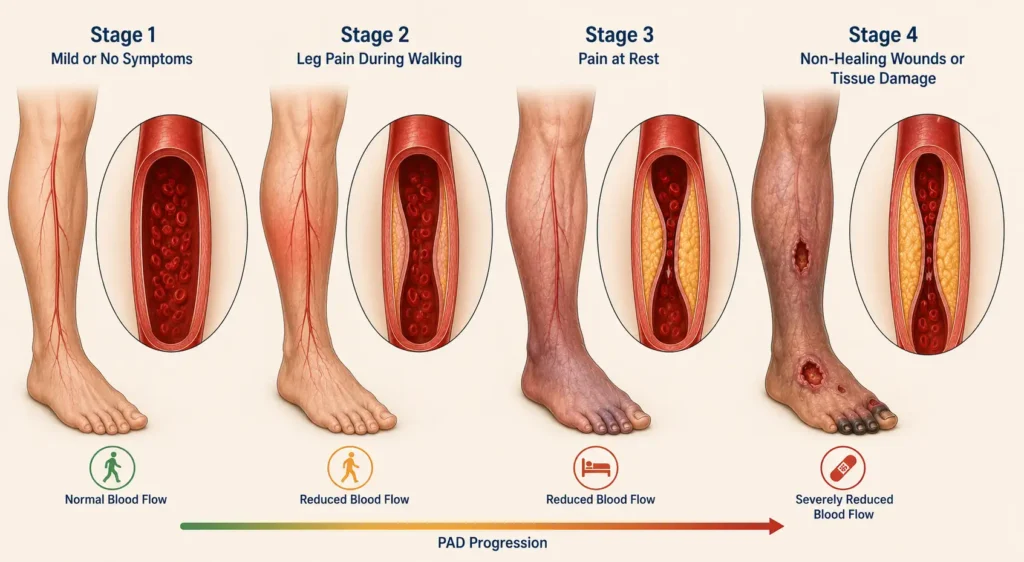
How Peripheral Artery Disease Develops (Pathophysiology)
Let me walk you through what actually happens inside your arteries. I promise this will make sense.
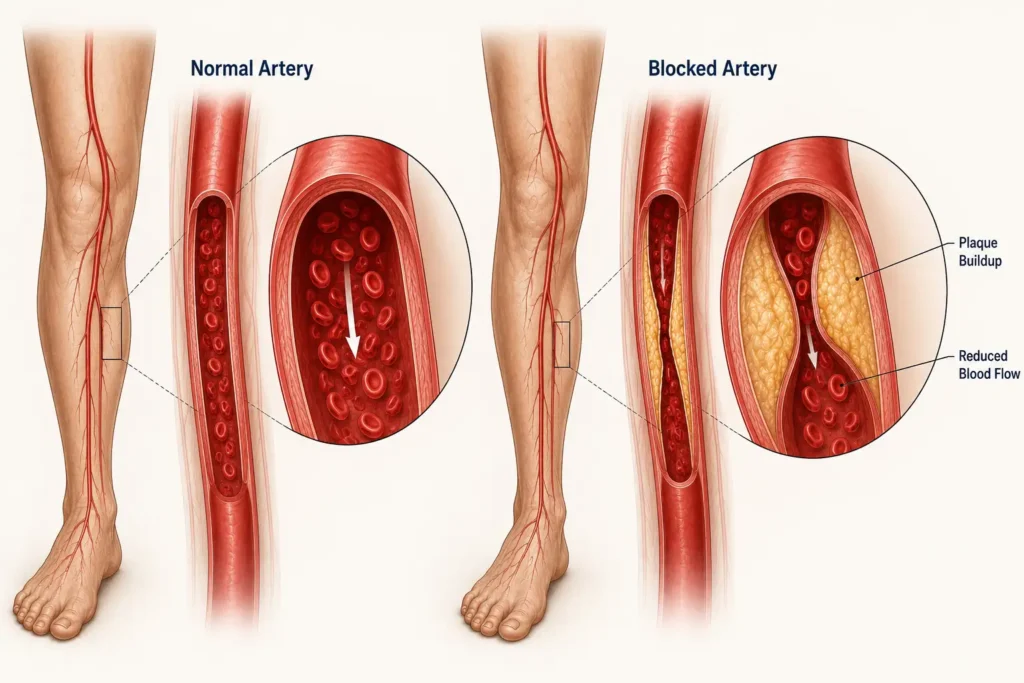
Think of a healthy artery like a smooth, flexible pipe. Its inner lining — called the endothelium — is remarkably thin, just one cell thick, but incredibly important. In poor circulation disease, this protective lining slowly becomes damaged over time. It normally keeps blood flowing smoothly and prevents anything from sticking to the artery walls.
Now, when risk factors like smoking, high blood sugar, high blood pressure, or elevated cholesterol are present over many years, this lining gets damaged. In Peripheral Artery Disease (PAD), the artery wall slowly becomes inflamed over time. And once inflammation sets in, LDL cholesterol — the bad kind — starts entering the artery wall.
Once inside the wall, LDL gets oxidized. The body sends immune cells to deal with it. These immune cells, called macrophages, swallow the oxidized LDL and become what we call foam cells. Over time, these foam cells accumulate and form what is called a plaque—a fatty, fibrous deposit inside the artery wall that plays a major role in PAD
As plaque grows, the artery becomes narrower. Blood flow decreases. When the narrowing exceeds around 60 percent, blood flow during physical activity becomes insufficient.
The muscles in your legs start receiving less oxygen than they need during exercise. This shortage of oxygen triggers peripheral artery disease symptoms, which is exactly where our next section begins.
Early Symptoms of Peripheral Artery Disease
This is the most important section of this entire article. Please read it carefully.

Peripheral Artery Disease (PAD) is deceptive. It develops slowly over years, and its early symptoms are easy to dismiss. People blame aging, tiredness, or muscle weakness — and the opportunity for early treatment is lost. Here is what Peripheral Artery Disease symptoms actually look like in the early stages.
Intermittent Claudication — The Defining Symptom
The word “claudication” comes from the Latin word for “limping”—and that is precisely what this symptom leads to over time.
Patients describe it as a cramping, aching, or heaviness in the calf muscles—sometimes the thighs or buttocks—that appears predictably when they walk and disappears within a few minutes of rest. Then they walk again, and it comes back. This pattern—pain with walking, relief with rest—is one of the most common Peripheral Artery Disease symptoms.
Why does this happen? When your leg muscles work during walking, they demand more oxygen. But the narrowed arteries cannot deliver enough blood to meet that demand.
The muscles shift to a backup energy process that produces lactic acid as a byproduct. That lactic acid buildup is what creates the pain. When you rest, the demand drops, lactic acid clears, and the pain goes away.
Many of my patients tell me they thought it was just “getting old.” I understand. But if your pain follows this precise pattern, where walking brings it on and rest relieves it, please do not ignore it.
Cold Foot or Cold Lower Leg
If one of your feet feels consistently colder than the other, that is not a coincidence. It may be one of the early Peripheral Artery Disease symptoms caused by reduced blood flow in the leg. This temperature difference is something a doctor can feel with their hands during examination. Patients often notice it themselves, especially at night.
Numbness or Heaviness in the Leg
Some patients describe a dull numbness or a heavy, tired sensation in one leg — not pain exactly, but a sense that the leg is not quite right. These Peripheral Artery Disease symptoms can occur because nerves and muscles are both affected by reduced blood supply. It may come and go, or it may be persistent.
Skin Changes: the Body Tells Its Own Story
Over time, inadequate blood supply changes the appearance of the skin on the legs. These are signs that many patients do not connect to their arteries at all:
- Shiny, tight-looking skin on the lower leg
- Loss of hair on the legs, particularly below the knee
- Skin that appears pale or bluish when the leg is raised
- Skin that turns dusky red when the leg is lowered
- Thickened or slow-growing toenails
These changes happen gradually, which is exactly why they go unnoticed for so long.
Slow-Healing Wounds or Sores on the Feet
This one worries me the most, especially in my diabetic patients. A small cut, a blister, or a minor abrasion on the foot should heal within seven to ten days in a healthy person. In a patient with Peripheral Artery Disease (PAD), blood flow is not sufficient to support the healing process. The wound lingers. It gets infected. And what started as a small sore can become a serious problem.
If you have a wound on your foot that has not healed in two weeks, please see a doctor — do not wait.
An Important Note for Diabetic Patients
I want to be very specific here because this group of patients is at especially high risk. If you have diabetes and have developed nerve damage, known as diabetic neuropathy, you may not feel the typical Peripheral Artery Disease symptoms at all. The nerves that carry pain signals are damaged, so the warning system does not function properly.
This is how PAD silently progresses in diabetic patients until a wound appears or blood flow becomes critically reduced. If you have diabetes and are above the age of 50, please ask your doctor about PAD screening regardless of whether you have leg pain or not.
Diagnosis of Peripheral Artery Disease
Diagnosing PAD does not always require expensive tests or hospital admission. A good clinical assessment and one simple bedside measurement can tell us a great deal.

Clinical History
The conversation matters enormously. When I sit with a patient, I ask very specific questions: How far can you walk before the pain starts? Which part of the leg hurts? Does it go away with rest? How quickly? Have you noticed any wounds that are slow to heal? Do you smoke or have diabetes?
The answers to these questions already paint a fairly clear picture before any test is done.
Physical Examination
I check the pulse at two specific points on the foot—the dorsalis pedis pulse on the top of the foot and the posterior tibial pulse at the inner ankle. A weak or absent pulse at either of these points is a significant finding. I also check skin temperature, look for any ulcers, and assess the color of the skin.
Ankle-Brachial Index—The Most Important Test
This is the test I want every patient to know about, because it is simple, painless, and remarkably accurate for detecting Peripheral Artery Disease symptoms.
We measure the blood pressure in the arm and then at the ankle using a blood pressure cuff and a small Doppler device. We divide the ankle pressure by the arm pressure. The result is the Ankle-Brachial Index, or ABI.
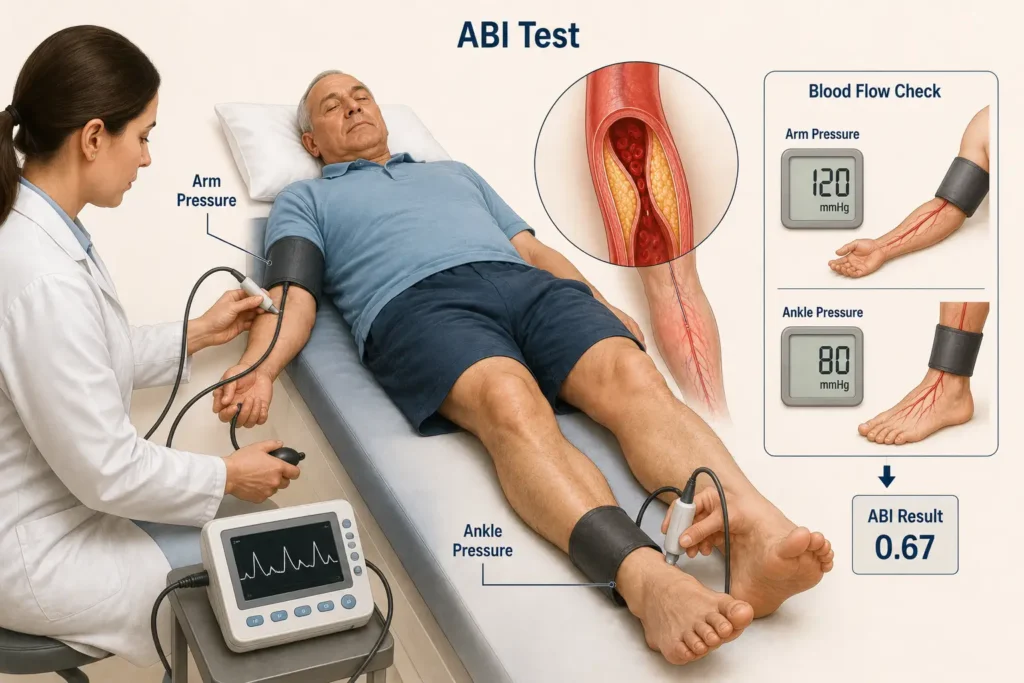
A normal ABI is between 1.0 and 1.4. An ABI below 0.90 confirms PAD. An ABI below 0.40 means the disease is severe and the limb may be at risk.
This test takes about ten minutes and is recommended by the American College of Cardiology and the American Heart Association as the primary screening tool for Peripheral Artery Disease (PAD).
Doppler Ultrasound
When we need to locate exactly where the narrowing is and how severe it is, we use a Doppler ultrasound. It shows us blood flow velocity and direction in specific arteries—without any needles or radiation.
Advanced Imaging—CT and MR Angiography
For patients who are being considered for surgical or procedural intervention, we use CT angiography or MR angiography to get a detailed map of the blood vessels. These are typically ordered when more conservative treatments are not working.
Evidence-Based Medical Management
Let me be clear: the goal of treatment is not just to manage Peripheral Artery Disease symptoms. The goal is to protect your heart and brain, slow the disease, and maintain the best possible quality of life. The major international guidelines, including those from the ACC/AHA (2016, updated 2021) and the European Society of Cardiology (2017), form the basis of everything I am about to describe.
Antiplatelet Therapy — Aspirin or Clopidogrel
Blood thinners in the antiplatelet category, primarily aspirin and clopidogrel, reduce the risk of blood clots forming in the narrowed arteries. They also reduce the risk of heart attacks and strokes. Multiple randomized controlled trials have confirmed their benefit in patients with Peripheral Artery Disease (PAD), and these medications are a cornerstone of treatment.
Statin Therapy — For Cholesterol and Much More
Statins are among the most well-studied medicines in all of cardiovascular medicine. In patients with Peripheral Artery Disease (PAD), we recommend high-intensity statins not just to lower LDL cholesterol but because statins also stabilize plaques, reduce arterial inflammation, and have been shown in multiple JAMA Cardiology studies and ACC consensus statements to reduce cardiovascular deaths.
I tell my patients: this tablet is protecting your heart as much as it is helping your leg.
Blood Pressure Control
The HOPE Trial published in 2000 was a landmark study showing that ACE inhibitors, a class of blood pressure medicines, significantly reduce cardiovascular events in high-risk patients, including those with vascular disease and Peripheral Artery Disease (PAD). Keeping blood pressure well controlled is non-negotiable in PAD management.
Diabetes Management
High blood sugar accelerates atherosclerosis. If you have diabetes, controlling your HbA1c, your three-month average blood sugar, is directly linked to how quickly Peripheral Artery Disease (PAD) progresses.
Some newer diabetes medications also have direct cardiovascular protective effects, which your doctor may consider depending on your specific situation.
Cilostazol — Improving Walking Distance
This medication works specifically to improve blood flow in the legs and has been shown in clinical trials to meaningfully increase the distance patients can walk before pain sets in.
It is used for intermittent claudication. However, it is contraindicated in patients with heart failure, so this decision always requires a doctor’s evaluation.
Supervised Exercise Therapy
This is a treatment option that patients are often surprised by. Structured, supervised walking exercise, performed three times per week with gradual progression, is one of the most effective interventions we have for improving walking distance in patients with Peripheral Artery Disease (PAD).
It encourages the growth of small alternative blood vessels around the blockages. It is not always easy in the early weeks, but the benefits are real and well-documented.
Risk Factors
- Smoking
- Diabetes
- High blood pressure
- High cholesterol
- Obesity
- Family history
- Lack of exercise
- Age above 50
When Is Revascularization Needed?
The majority of patients with Peripheral Artery Disease (PAD), especially those with mild to moderate disease, can be managed effectively with medicines and lifestyle changes. Surgery or a procedure is not the first step. But there are specific situations where we intervene.

Indications for Intervention
- Claudication that severely limits daily activities despite optimal medical therapy
- Critical limb-threatening ischemia, meaning the leg is not getting enough blood even at rest
- Rest pain, which is constant pain in the foot even when lying down and often becomes worse at night
- Non-healing ulcers or wounds on the foot
- Gangrene or tissue loss
What the Procedure Involves
The less invasive option is balloon angioplasty—a catheter is guided into the narrowed artery and a small balloon is inflated to open it up. Sometimes a metal stent is placed to keep the artery open. These are done through a small puncture in the groin or wrist, without major surgery, and patients often go home the next day.
When blockages are long or complex, surgical bypass may be needed—creating a detour route for blood to travel around the blocked segment.
The decision between angioplasty and bypass depends on the location, length, and nature of the blockage, as well as the patient’s overall health. It is always individualized.
Global Mortality and Impact
I think it is worth stepping back and looking at the big picture one more time, because the numbers are sobering.
According to the GBD 2019 data, Peripheral Artery Disease (PAD) contributes significantly to global cardiovascular mortality, and the impact is not evenly distributed.
Patients in low-resource settings have considerably worse outcomes, not because the disease is inherently different, but because they have less access to early screening, medications, and specialist care.
The regions carrying the highest burden of Peripheral Artery Disease (PAD) are South Asia and Sub-Saharan Africa. And critically, most deaths in PAD patients are not caused by the leg disease itself—they are caused by heart attacks and strokes, which reflects exactly what I said at the beginning: PAD is a window into the health of your entire cardiovascular system.
In higher-income regions like North America and Western Europe, improved awareness and cardiovascular risk management have helped reduce mortality rates over the past two decades.
This shows clearly that outcomes can be changed when the disease is caught early and treated properly.
Global Distribution Map
Based on the GBD 2019 data and WHO cardiovascular reports, the global distribution of PAD burden looks roughly like this:
High Prevalence Regions
- South Asia — including India, Pakistan, Bangladesh
- Sub-Saharan Africa — driven by limited healthcare access and high smoking rates
- Eastern Europe — where cardiovascular risk factors remain poorly controlled
Moderate Prevalence
- North America — high awareness, but aging population keeps numbers significant
- Western Europe — better managed but still substantial
Lower Reported Prevalence
- East Asia — though underdiagnosis may account for some of this difference
Note: A visual infographic map showing these regions is recommended for web display.
Prevention
Let me be direct: most cases of PAD are preventable. The risk factors are well-known, and addressing them, even partially, makes a significant difference. Here is what actually works:

Stop Smoking
If there is one single thing that matters most, it is this. Smoking is the most powerful modifiable risk factor for Peripheral Artery Disease (PAD). It damages artery walls, accelerates plaque formation, and constricts blood vessels.
Quitting smoking, at any age, slows the progression of the disease. If you are still smoking and have PAD, this is the most important conversation to have with your doctor.
Control Your LDL Cholesterol
High LDL is the fuel for plaque formation. Getting it to target levels through diet, exercise, and statins is one of the most evidence-based interventions in cardiovascular medicine. Your doctor will tell you your specific target based on your overall risk.
Keep Your Blood Sugar in Check
For diabetic patients, every percentage point decrease in HbA1c reduces the risk of vascular complications. This is not abstract — it translates directly into slower disease progression and fewer complications.
Exercise Regularly
Walking — yes, even with some discomfort in early PAD — is therapeutic. Aim for at least 30 minutes of walking most days of the week. Supervised exercise programs are available at many cardiac rehabilitation centers. The benefits are well-documented and the cost is essentially zero.
Screen High-Risk Individuals
If you are above the age of 50 and have any combination of smoking history, diabetes, high blood pressure, or high cholesterol, ask your doctor about Peripheral Artery Disease (PAD) screening and an ABI test. It is simple, painless, and could catch the disease years before it becomes a serious problem.
Frequently Asked Questions (FAQ)
Is PAD curable?
Not fully, but very manageable. With medicines and lifestyle changes, most patients live normal, active lives.
Does PAD increase heart attack risk?
Yes—2 to 3 times higher. PAD reflects blockages throughout the body, so we treat the whole cardiovascular system, not just the leg.
Who should get screened for Peripheral Artery Disease (PAD)?
Adults over 50 with diabetes, smoking history, high blood pressure, or high cholesterol should be screened for PAD. If you have leg pain while walking, get checked regardless of age—PAD can occur earlier in high-risk individuals.
Is surgery always needed for PAD?
No. Most cases are managed with medicines and exercise. Surgery is only for severe cases critical blockages or non-healing wounds.
Can I exercise with PAD?
Yes, and you should. Walking regularly is actually part of the treatment. Start slow, build up, and always check with your doctor first.
Can cold feet be a symptom of Peripheral Artery Disease?
Yes, persistent coldness in one foot, especially compared to the other, can be an early warning sign of PAD. A simple Ankle-Brachial Index (ABI) test can confirm or rule out PAD in about 10 minutes.
Can PAD affect both legs?
Yes, PAD can affect one or both legs depending on which arteries are narrowed.
Conclusion
Peripheral Artery Disease (PAD) is serious but manageable. Recognize the warning signs early: leg pain while walking, cold feet, or slow-healing wounds. These are your body’s signals — don’t ignore them.
Most people with PAD live full, active lives with the right treatment. Surgery is rarely the first answer.
If you notice any of these signs, don’t wait. A simple ABI test could protect not just your legs but your heart and your life.
Medical Disclaimer
This article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider regarding symptoms or medical conditions.
About the Author
Iraphan Khan, BSN | D.Pharm | CMLT, is a Healthcare SEO Strategist and Medical Content Writer at RealMedVision, creating clinically accurate content optimized for Google and AI search.
Medically Reviewed By
Dr Praveen Verma MBBS MD — Diagnostic & Pathology
Dr Himanshu Morya MBBS — Clinical Accuracy & Patient Safety
Kalpna Singh Shekhawat BSN NP — Patient Care & Practical Accuracy
References:
1. World Health Organization (WHO). Cardiovascular Diseases (CVDs) Fact Sheet
2. American Heart Association (AHA). Peripheral Artery Disease (PAD)
3. National Heart, Lung, and Blood Institute (NHLBI). Peripheral Artery Disease
4. Mayo Clinic. Peripheral Artery Disease (PAD)
5. Cleveland Clinic. Peripheral Artery Disease (PAD)
6. American College of Cardiology (ACC) / American Heart Association (AHA). 2024 Guideline for Lower Extremity Peripheral Artery Disease
7. European Society of Cardiology (ESC). Peripheral Arterial Diseases Guidelines
8. Global Burden of Disease (GBD) Study 2019. The Lancet Global Health Data
9. JAMA Cardiology. Cardiovascular Risk in Patients With Peripheral Artery Disease
10. Harvard Medical School. Atherosclerosis and Vascular Disease Research
11. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine (12th Edition). Elsevier.
12. Harrison’s Principles of Internal Medicine (21st Edition). McGraw-Hill Education.
13. Society for Vascular Surgery (SVS)
14. Johns Hopkins Medicine. Peripheral Artery Disease (PAD)
15. NIH MedlinePlus. Peripheral Arterial Disease