
How a Childhood Throat Infection Can Quietly Destroy Your Heart During Pregnancy
What Most Pregnant Women Never Know Until the Heart Starts Failing
A patient-friendly guide by RealMedVision
Last Update—May 2026

Key Takeaways
Rheumatic Heart Disease in Pregnancy is a serious but often underdiagnosed heart condition. It develops when untreated childhood throat infections permanently damage heart valves.
Early symptoms are often mistaken for normal pregnancy changes. With early diagnosis and specialist care, most women can have a safe pregnancy and healthy delivery.
Introduction
Pregnancy brings a lot of joy—but for women with Rheumatic Heart Disease in Pregnancy, it can quietly become one of the most dangerous times of their life.
The difficult truth is this. Most women do not even know their heart valves are damaged. Years ago, as a child, they had a sore throat. It was ignored. No antibiotics. No follow-up. Life went on. But inside the heart, the damage was slowly happening.
Now, pregnant, the body is asking the heart to do much more than usual. And a heart with damaged valves may not be able to keep up.
According to the World Health Organization (WHO), Rheumatic Heart Disease affects over 40 million people worldwide. It remains the most common cause of heart disease in pregnant women across South Asia, Sub-Saharan Africa, and parts of Latin America.
But here is the important part. Rheumatic Heart Disease in Pregnancy does not have to end badly. When it is caught early and managed properly, most women go through pregnancy safely and deliver healthy babies.
The real danger is not knowing about it at all.
What You Will Learn
In this article, you will learn:
- What Rheumatic Heart Disease is and how it develops
- Why pregnancy increases the risk of complications
The 7 early symptoms every pregnant woman should know
- Risks for both the mother and the baby
- How doctors diagnose Rheumatic Heart Disease in Pregnancy
- Available treatment and management options
- Home care and lifestyle tips that can help
- When symptoms become a medical emergency
- How early diagnosis can improve outcomes for mother and baby
Everything is written in simple, clear language—because this information can genuinely save a life.
What Is Rheumatic Heart Disease in Pregnancy?
Rheumatic Heart Disease in Pregnancy becomes easier to understand when you know how this condition actually starts—because the beginning has nothing to do with the heart directly.
It starts with a simple throat infection in childhood.
A child gets a sore throat caused by Streptococcal bacteria (a type of harmful germ that causes throat infections). In most cases, antibiotics treat it completely. No lasting damage.
But when this infection goes untreated, something goes wrong inside the immune system (the body’s natural defense system). The body starts attacking its own heart valves by mistake—because the valves look similar to the bacteria it is trying to fight. This abnormal attack is called Rheumatic Fever.
After repeated episodes of Rheumatic Fever over years, the heart valves get permanently scarred. They may become stiff and narrow—making it hard for blood to pass through. This is called Stenosis (narrowing). Or they may become loose and leaky—letting blood flow backward. This is called Regurgitation (backward leaking).
The mitral valve (the valve between the left upper and lower chambers of the heart) is the most commonly damaged valve in Rheumatic Heart Disease.
This is not a Heart Attack. This is not a blocked artery. This is structural valve damage—and it stays for life unless surgically corrected.
Why Pregnancy Makes Rheumatic Heart Disease So Dangerous
During pregnancy, the body makes dramatic changes to support the growing baby.
Blood volume (total amount of blood inside the body) increases by up to 50 percent. The heart rate goes up. The heart pumps significantly more blood every minute than it normally does. These changes peak during the third trimester and become most intense during labor itself.
For a woman with healthy heart valves, the heart handles all of this without difficulty.
But for a woman with Rheumatic Heart Disease—especially one with a narrowed or leaking mitral valve—this extra demand creates a dangerous situation. The heart is being pushed to do more work through a valve that is already damaged and struggling.
Pressure builds up. Fluid starts backing up into the lungs. The heart begins to strain in ways it cannot safely handle.
The CDC reports that cardiac disease—including Rheumatic Heart Disease—is now among the leading indirect causes of maternal death in both developing and developed countries.
In India, ICMR data shows that Rheumatic Heart Disease in Pregnancy remains a major cause of pregnancy-related cardiac complications, particularly among women under 35.
Types of Valve Problems in Rheumatic Heart Disease
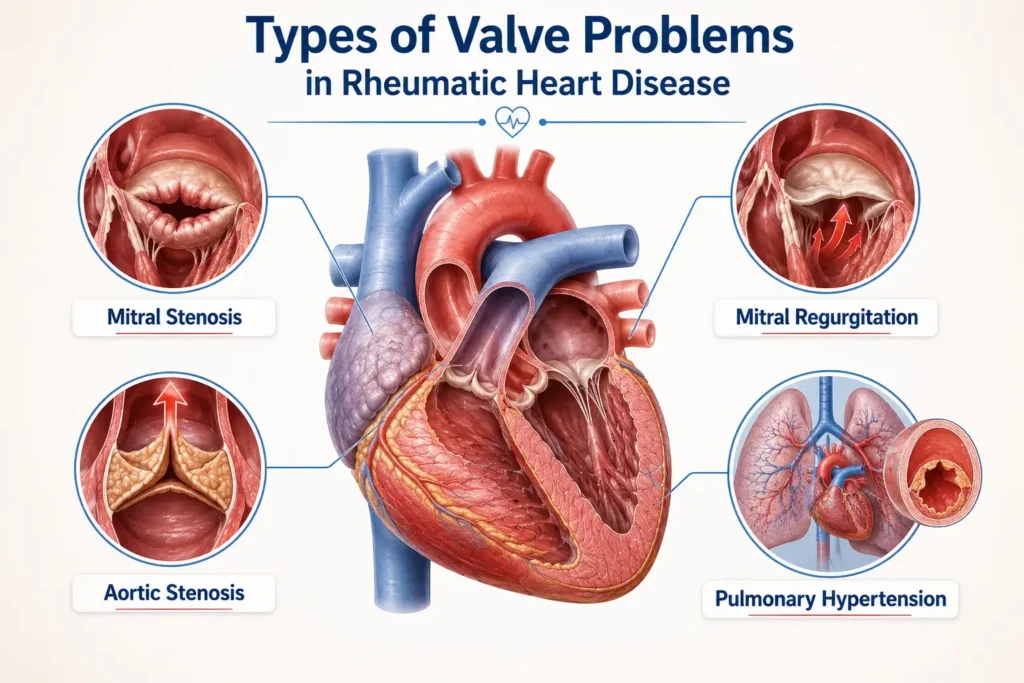
Understanding which valve is damaged matters a lot—because different damage carries different levels of risk during pregnancy.
Mitral Stenosis
(Narrowing of the mitral valve) is the most dangerous problem during pregnancy. As blood volume increases, the narrowed valve creates a bottleneck.
Fluid backs up into the lungs and can cause Pulmonary Edema (dangerous fluid in the lungs—a life-threatening emergency). Severe Mitral Stenosis carries the highest risk of all valve conditions in pregnancy.
Mitral Regurgitation
(Leaking of the mitral valve—blood flows backward with each heartbeat) is generally better tolerated during pregnancy. But moderate to severe cases still need careful monitoring throughout all nine months.
Aortic Valve Disease
particularly Aortic Stenosis (narrowing of the aortic valve—the valve that controls blood leaving the heart to the whole body) carries serious risk when severe. The heart simply cannot meet the increased demands of pregnancy through a critically narrowed outlet.
Pulmonary Hypertension
(High blood pressure in the lung blood vessels) can develop as a complication of longstanding Rheumatic Heart Disease and makes pregnancy particularly high risk.
7 Early Symptoms of Rheumatic Heart Disease in Pregnancy
This is where Rheumatic Heart Disease in Pregnancy becomes most dangerous—because many early symptoms look exactly like normal pregnancy changes. Breathlessness, fatigue, and a faster heartbeat can all feel like a natural part of pregnancy. This overlap is exactly why so many cases are missed until things get serious.
Based on CDC cardiac disease in pregnancy guidelines and WHO maternal health recommendations, these are the 7 early symptoms every pregnant woman and her family must know:

Symptom 1: Breathlessness at Rest
Breathlessness at Rest Normal pregnancy breathlessness happens during walking or climbing stairs. But breathlessness while just sitting, talking, or lying down is not normal. If a pregnant woman is struggling to breathe without any physical effort, this needs immediate medical attention.
Symptom 2: Heart Racing or Pounding That Feels Unusual
Heart Racing or Pounding That Feels Unusual Some increase in heart rate is normal in pregnancy. But a heart that races suddenly, flutters, or pounds without reason—especially at rest—is a red flag. This could indicate Arrhythmia (irregular heart rhythm) developing because of valve pressure.
Symptom 3: Swelling in Legs, Ankles, or Feet That Is Getting Worse
Swelling in Legs, Ankles, or Feet That Is Getting Worse Mild ankle swelling is common in pregnancy, especially in the evenings. But swelling that keeps getting worse, affects both legs all day, and does not improve with rest can be a sign that the heart is not pumping efficiently enough.
Symptom 4: Chest Tightness or Discomfort
Chest Tightness or Discomfort Any chest discomfort in pregnancy should be taken seriously. In Rheumatic Heart Disease in Pregnancy, this can feel like pressure or tightness—similar to what is described in Angina (chest pain caused by reduced blood flow to the heart muscle). It should never be dismissed as gas or acidity without proper evaluation.
Symptom 5: Extreme Fatigue That Feels Disproportionate
Extreme Fatigue That Feels Disproportionate Pregnancy is tiring—everyone knows this. But fatigue so severe that simple activities like bathing or cooking feel exhausting is not normal tiredness. This is the kind of fatigue that comes from a heart working far harder than it should.
Symptom 6: Waking Up At Night Unable to Breathe
Waking Up At Night Unable to Breathe Waking up suddenly at night gasping for air—and needing to sit up or open a window to breathe—is called Orthopnea (difficulty breathing when lying flat). This is one of the most classic signs of fluid starting to back up near the lungs, and it is a serious warning sign of Rheumatic Heart Disease.
Symptom 7: A Persistent Cough, Especially at Night
A Persistent Cough, Especially at Night A dry, nagging cough that shows up mostly when lying down—and does not go away despite no cold or infection—can be caused by fluid building up near the lung tissue. A pink or frothy cough is a late and very serious sign that needs emergency care immediately.
Causes and Risk Factors
The direct cause of Rheumatic Heart Disease is untreated or repeatedly undertreated Streptococcal throat infections during childhood.
In India and many lower-income regions, limited access to antibiotics and poor follow-up care means many children experience repeated episodes of Rheumatic Fever without proper treatment.
Risk factors that can make Rheumatic Heart Disease in Pregnancy more dangerous include:
- Severe valve narrowing (especially Mitral Stenosis)
- Previous history of heart failure
- Pulmonary Hypertension (high pressure in the lung blood vessels)
- Atrial Fibrillation (an irregular and often rapid heart rhythm)
- Anemia (low iron and low red blood cell levels)
- Poorly controlled infections during pregnancy
- Limited or no access to regular antenatal care
- Delayed diagnosis of heart valve disease
The UNFPA has identified maternal cardiac disease as a major indirect cause of maternal mortality in developing countries. Women with multiple risk factors often require specialist cardiac and obstetric care throughout pregnancy.
How the Disease Damages the Heart
Think of the heart as a one-way water pump with gates (valves) that open and close at just the right time to keep blood flowing in the right direction.
Mitral Stenosis
In Mitral Stenosis, the main gate becomes too narrow. The pump has to push much harder to force blood through. During pregnancy, when blood volume is up by 50 percent, this narrow gate becomes a critical danger point.
Fluid backs up behind it. The Ejection Fraction (the percentage of blood the heart pumps out with each beat—normal is 55 to 70 percent) can drop significantly in advanced cases.
Mitral Regurgitation
In Mitral Regurgitation, the gate does not close properly. Blood leaks backward with every beat. The heart wastes energy pushing the same blood in a circle instead of sending it forward to the body and baby.
Why Pregnancy Makes It More Dangerous
Both problems become dramatically more dangerous during pregnancy because the heart has no reserve left to handle the extra demand.
Diagnosis During Pregnancy
The good news is that diagnosing Rheumatic Heart Disease in Pregnancy is safe, straightforward, and does not require anything risky for the baby.
ECG Test
(Electrocardiogram—a test that records the heart’s electrical activity using small stickers placed on the skin) is usually done first.
It can detect irregular heart rhythms, signs of valve strain, and evidence of Atrial Fibrillation. An abnormal ECG Test result always needs further investigation in a pregnant woman.
2D Echo
2D Echo (Two-Dimensional Echocardiogram — a heart ultrasound that uses sound waves to show the heart’s structure and movement in real time) is the most important test for Rheumatic Heart Disease.
It shows exactly which valve is damaged, how severe the narrowing or leaking is, and whether the Ejection Fraction is normal.
It uses no radiation and is completely safe in pregnancy. Both WHO and Indian obstetric guidelines recommend 2D Echo as the first-line investigation for any pregnant woman with suspected cardiac disease.
Blood Tests
Blood Tests check for anemia (low iron), heart stress markers, kidney function, and oxygen levels—all of which directly guide treatment decisions.
Normal Blood Pressure Monitoring
Normal Blood Pressure monitoring is important throughout pregnancy—consistently elevated blood pressure on top of valve disease significantly increases the risk of complications.
According to the Cleveland Clinic, early echocardiographic (2D Echo-based) diagnosis of valve disease in pregnancy significantly improves outcomes for both mother and baby.
Treatment Options
Treatment of Rheumatic Heart Disease depends on which valve is affected, how severe the damage is, and the stage of pregnancy.
Mild Cases
Mild cases are often managed with regular monitoring, reduced salt intake, iron supplementation for Anemia, and frequent cardiology and obstetric follow-up visits.
Moderate to Severe Cases
More severe cases may require medicines. Diuretics (water tablets) help remove excess fluid, Beta-blockers reduce strain on the heart, and Anticoagulants (blood thinners) may be needed in selected women with Atrial Fibrillation or mechanical heart valves.
Balloon Mitral Valvotomy
Balloon Mitral Valvotomy (a procedure used to widen a narrowed mitral valve) may be performed during the second trimester when severe Mitral Stenosis becomes life-threatening and does not respond to medicines.
Managing Other Heart Conditions
Conditions such as Pericarditis, if diagnosed and treated early, can help prevent additional cardiac complications during pregnancy.
Can Pregnancy Be Continued Safely?
According to WHO and CDC guidelines, pregnancy termination should not be automatically recommended for women with Rheumatic Heart Disease. With proper specialist care, many women can complete pregnancy safely and deliver healthy babies.
Risks to the Baby
Rheumatic Heart Disease in Pregnancy can affect both the mother and baby. Poor heart function may reduce the oxygen and nutrients reaching the baby.
Possible Risks to the Baby
PAHO research has shown that untreated maternal cardiac disease increases the risk of:
- Premature birth (baby born before 37 weeks)
- Low Birth Weight (baby weighing less than 2.5 kilograms at birth)
- Fetal growth restriction (baby not growing at the right rate inside the womb)
- Fetal distress during labor
Fetal monitoring—alongside maternal cardiac monitoring—is a standard part of managing Rheumatic Heart Disease at specialist centers.
Home Care Tips
While medicines and specialist care are important, daily habits also play a key role.
- Weigh yourself every morning. Sudden weight gain may indicate fluid buildup.
- Sleep with your head slightly elevated if nighttime breathlessness occurs.
- Reduce salt intake to help control swelling and fluid retention.
- Rest when needed and avoid overexertion.
- Keep a simple symptom diary and discuss any changes with your doctor.
Lifestyle Changes That Help
- Avoid heavy physical activity that causes breathlessness or chest discomfort.
- Light walking may be helpful if approved by your cardiologist.
- Quit smoking completely.
- Manage stress through breathing exercises and adequate sleep.
- Avoid very hot environments and strenuous household work, especially during the third trimester.
Diet Tips
- Reduce salt intake to less than 2 grams per day to help control fluid retention.
- Eat iron-rich foods such as spinach, lentils, and dates to prevent Anemia.
- Include plenty of fruits, vegetables, and whole grains in your diet.
- Avoid processed and packaged foods because they often contain hidden salt.
- Stay hydrated, but follow your doctor’s advice if fluid restriction is recommended.
- Foods rich in Magnesium, such as bananas, nuts, and seeds, may help support a healthy heart rhythm.
According to ICMR nutrition guidelines, low-sodium diets and adequate iron intake are especially important for women with Rheumatic Heart Disease in Pregnancy.
Complications
When Rheumatic Heart Disease goes unmanaged, serious complications can develop, especially during the third trimester and labor when the heart is under maximum stress.
Possible Complications
- Acute Heart Failure (the heart cannot pump enough blood for the mother and baby)
- Pulmonary Edema (dangerous fluid buildup in the lungs)
- Stroke caused by blood clots
- Dangerous Arrhythmia (abnormal heart rhythm)
- Maternal death in severe untreated cases
These are real risks documented by the AHA and WHO in women who did not receive specialist cardiac care during pregnancy.
The good news is that with early diagnosis and proper specialist management, many of these complications can be prevented or successfully treated.
Prevention
Prevention of Rheumatic Heart Disease begins in childhood and continues through pregnancy.
In Childhood
- Treat Streptococcal throat infections promptly with antibiotics.
- Children with a history of Rheumatic Fever may require long-term Penicillin prophylaxis to prevent further valve damage.
Before Pregnancy
- Women with known Rheumatic Heart Disease should have a detailed 2D Echo before planning pregnancy.
- Severe valve disease should be evaluated and treated before conception whenever possible.
- Pregnancy planning should involve both a cardiologist and an obstetrician.
During Pregnancy
- Attend all antenatal appointments.
- Avoid heavy physical exertion.
- Manage Anemia and infections promptly.
- Monitor normal blood pressure throughout pregnancy.
Know Emergency Symptoms
Heart Attack Symptoms such as sudden chest pain, heavy sweating, jaw pain, or severe breathlessness should always be treated as a medical emergency, even during pregnancy.
When to See a Doctor
See a cardiologist immediately if you are pregnant and experience:
- Unexplained breathlessness
- Worsening leg swelling
- Heart racing without reason
- Chest discomfort or chest pain
This is especially important if you have a history of Rheumatic Fever or a heart murmur.
WHO maternal health guidelines recommend that women with known heart disease consult a cardiologist before pregnancy so that valve disease can be assessed and a safe management plan can be created.
Do not wait for symptoms to improve on their own. Rheumatic Heart Disease in Pregnancy can worsen quickly without proper medical care.
Emergency Warning Signs
Seek emergency medical care if you experience:
- Severe breathlessness
- Fainting or loss of consciousness
- Crushing chest pain
- A very fast or irregular heartbeat
- Coughing up pink or frothy fluid
- Sudden severe swelling of the legs or face
These symptoms may indicate a life-threatening emergency and should never be ignored.
Prognosis and Recovery
The outlook for Rheumatic Heart Disease in Pregnancy depends on the severity of valve damage and how early treatment begins.
Women with mild to moderate disease who receive regular specialist care often have safe pregnancies and healthy babies. Those with severe Mitral Stenosis or Pulmonary Hypertension face higher risks but can still achieve good outcomes with expert management.
According to Johns Hopkins Medicine, regular follow-up, proper treatment, and delivery in a hospital with cardiac support significantly improve outcomes.
The biggest risk is not the diagnosis itself—it is delayed diagnosis and lack of specialist care.
Frequently Asked Questions (FAQs)
Q:1 Is pregnancy safe with mild Rheumatic Heart Disease?
Yes—with proper monitoring and regular specialist follow-up, most women with mild Rheumatic Heart Disease in Pregnancy can complete pregnancy safely and deliver healthy babies. The key is that “mild” must be confirmed by 2D Echo — not assumed. Mild on clinical examination can sometimes be moderate or severe on echocardiography.
Q:2 Can a woman with Rheumatic Heart Disease deliver normally?
Many women with Rheumatic Heart Disease in Pregnancy can have a vaginal delivery. A caesarean section is not automatically required. The decision depends on the severity of valve disease, how pregnancy has progressed, and cardiac status at the time of delivery. This decision must always be made jointly by a cardiologist and an obstetrician—not by a general practitioner alone.
Q:3 Is Rheumatic Heart Disease curable?
The valve damage caused by Rheumatic Heart Disease is permanent and cannot be reversed by medicines. However, symptoms can be effectively controlled. In cases of severe narrowing, surgical valve repair or balloon procedures can significantly improve valve function and quality of life—including making future pregnancy safer.
Q:4 Can Rheumatic Heart Disease be prevented?
Yes—and this is one of the most critical public health messages around this disease. Treating Streptococcal throat infections promptly with antibiotics in childhood completely prevents Rheumatic Fever, which in turn prevents Rheumatic Heart Disease. This is a disease that simply does not have to happen.
Q:5 Is Rheumatic Heart Disease common in India?
Yes. India continues to carry one of the highest burdens of Rheumatic Heart Disease globally — particularly among younger women in rural areas with limited access to early healthcare. ICMR data confirms it remains an important maternal cardiac health concern across multiple Indian states.
Q:6 What is the risk to the baby if the mother has Rheumatic Heart Disease in Pregnancy?
When the heart cannot pump efficiently, the baby may receive less oxygen and nutrition through the placenta. This increases the risk of premature birth, low birth weight, and fetal growth restriction. Regular fetal monitoring alongside cardiac monitoring is essential in all cases of Rheumatic Heart Disease in Pregnancy.
Q:7 Can Rheumatic Heart Disease Get Worse During Pregnancy?
Yes, it can. Pregnancy naturally increases blood volume and makes the heart work harder than usual. If a woman already has Rheumatic Heart Disease, especially severe Mitral Stenosis or Pulmonary Hypertension, symptoms may become worse as pregnancy progresses. Breathlessness, swelling, fatigue, and heart rhythm problems can become more noticeable during the second and third trimesters. Regular follow-up with both a cardiologist and obstetrician is important to detect complications early and keep both mother and baby safe.
Medical Disclaimer
This article is written purely for general educational awareness. It does not serve as medical advice, a diagnosis, or a treatment recommendation of any kind.
Pregnant women with known or suspected heart disease must consult a qualified cardiologist and obstetric specialist for personalized evaluation and care. Do not delay seeking emergency help if severe symptoms are present. In an emergency, call 112 immediately.
About the Author
Iraphan Khan, BSN | D.Pharm | CMLT, is a Healthcare SEO Strategist and Medical Content Writer at RealMedVision, creating clinically accurate content optimized for Google and AI search.
Medically Reviewed By
Dr Praveen Verma, MBBS, MD — Diagnostic & Pathology
Dr Himanshu Morya MBBS — Clinical Accuracy & Patient Safety
Kalpna Singh Shekhawat BSN NP — Patient Care & Practical Accuracy
References & Sources:
1.World Health Organization (WHO) — Rheumatic Heart Disease Global Data
2. American Heart Association (AHA) — Heart Valve Disease During Pregnancy
3. Centers for Disease Control and Prevention (CDC) — Cardiac Disease in Pregnancy
4. Indian Council of Medical Research (ICMR) — Rheumatic Heart Disease in India
5. Cleveland Clinic — Rheumatic Heart Disease Diagnosis and Treatment
6. Johns Hopkins Medicine — Heart Disease and Pregnancy
7. Mayo Clinic — Rheumatic Fever and Heart Valve Damage
8. NHS UK — Heart Conditions and Pregnancy
9. ACC/AHA Valvular Heart Disease Guidelines 2021 — Management During Pregnancy
10. PubMed (NIH National Library of Medicine) — Rheumatic Heart Disease in Pregnancy Research