
How Aortic Regurgitation Silently Damages Your Heart
Severe aortic regurgitation can silently damage the heart before symptoms appear. Learn why early surgery improves survival and heart recovery.
A patient-friendly guide by RealMedVision
Last Update – May 2026
Aortic regurgitation is a condition where the heart’s aortic valve leaks blood backward with every beat. Many patients feel completely normal for years while serious damage builds silently inside the heart. Early surgery for aortic regurgitation, before symptoms appear, is often what saves lives and protects long-term heart function.
Severe aortic regurgitation can silently damage the heart for years before a single symptom appears. Early surgery for aortic regurgitation often protects long-term heart function, improves survival rates, and prevents irreversible heart failure. Regular echocardiography is the single most important tool for catching dangerous progression before it becomes permanent.
What You Will Learn in This Guide
- What aortic regurgitation is and how a leaking aortic valve affects the heart
- How common aortic regurgitation is worldwide and who is most at risk
- The early, silent, and emergency symptoms patients should never ignore
- Main causes including bicuspid aortic valve, rheumatic heart disease, and aortic root disorders
- Risk factors that increase the chances of developing severe aortic regurgitation
- Different types, severity stages, and disease progression over time
- How chronic volume overload and left ventricular enlargement develop silently
- Why cardiologists sometimes recommend surgery before symptoms appear
- How doctors decide the right timing for aortic valve replacement surgery
- How echocardiography, cardiac MRI, and other tests diagnose the condition
- All treatment options including monitoring, medications, valve repair, and valve replacement
- What happens if severe aortic regurgitation is left untreated for too long
- Recovery, long-term prognosis, and life expectancy after valve surgery
- Diet, exercise, lifestyle changes, and prevention strategies
- Warning signs that mean you should see a doctor immediately
- Latest medical research, expert insights, and patient FAQs
Introduction
Let me tell you something that surprises most patients when they first hear it.
You can have a seriously leaking heart valve, measurable enlargement of your heart, and real damage building inside your chest — and still feel completely fine. No chest pain. No breathlessness. No warning at all.
That is what makes aortic regurgitation different from most heart conditions. It is quiet. Deceptively quiet.
I have spoken with patients diagnosed entirely by accident — during a routine checkup for something unrelated. A doctor listened, heard a murmur, ordered an echocardiogram, and suddenly a condition progressing silently for years came into full view.
Many patients say the hardest part emotionally is hearing that surgery may be needed while they still feel completely healthy. That confusion is completely understandable. The damage often travels far ahead of the symptoms.
What worries cardiologists most is not the patient who arrives breathless and exhausted. It is the patient who walks in feeling normal — because by the time symptoms finally show up, the damage is often already serious.
This article is about understanding why early surgery for aortic regurgitation can genuinely change outcomes. Not because surgery is always the answer—but because in this condition, timing matters more than most people realize.
What Is Aortic Regurgitation?
Your heart has four valves. Each one opens and closes with every heartbeat to keep blood moving in the right direction.
The aortic valve sits between the heart’s main pumping chamber—the left ventricle and the aorta, the body’s largest artery. Every time the heart beats, this valve opens to let blood through, then closes tightly to stop any from flowing back.
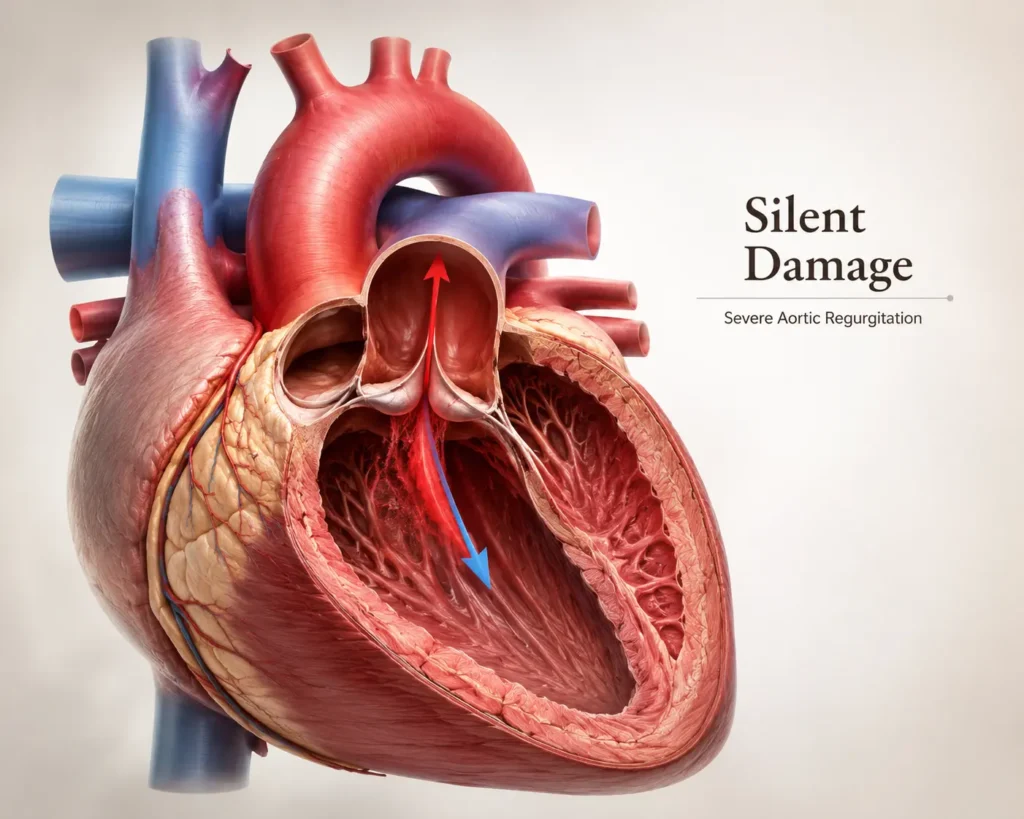
In aortic regurgitation — also called aortic insufficiency — that valve does not close properly. Blood leaks backward into the left ventricle after every single beat.
Think of it this way. Your heart pumps out a full cup of blood. But because the valve is leaking, a portion comes straight back. Now the ventricle must pump its normal load plus everything that returned. Every beat. Every minute. Every day.
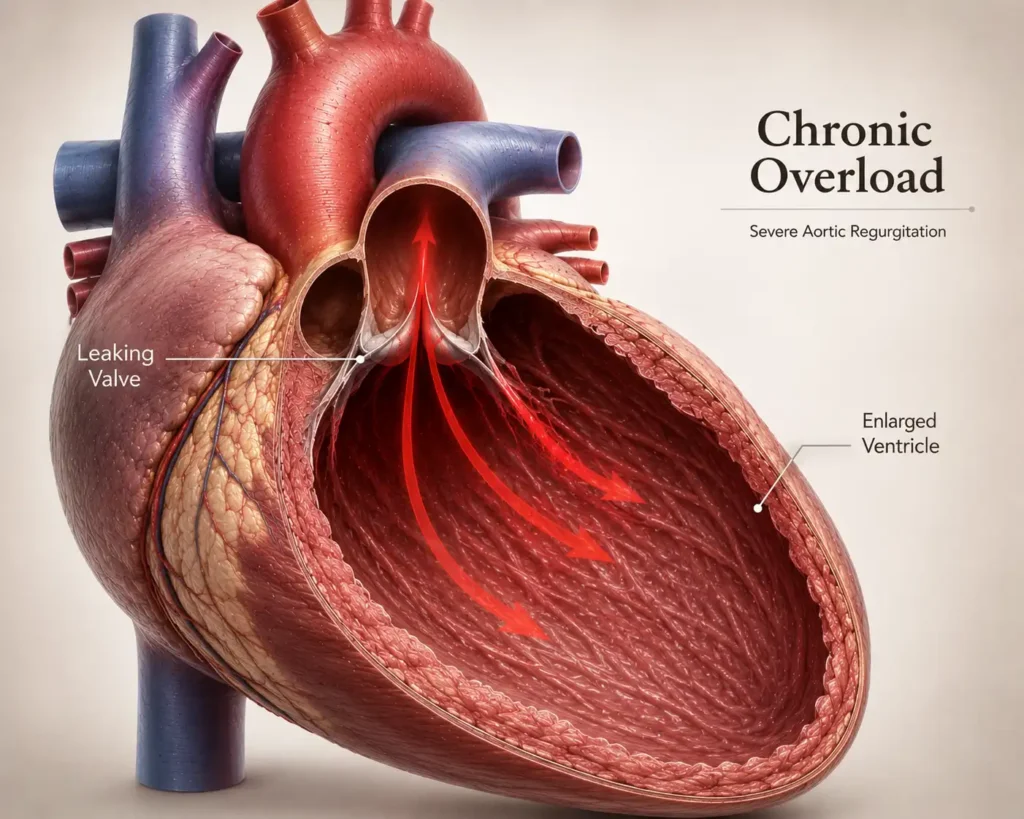
Over time, this extra work stretches and enlarges the left ventricle. For a while, the heart adapts. Eventually, that adaptation reaches its limit—and the heart begins to weaken.
The critical problem is that patients often feel none of this happening.
Summary:
Aortic regurgitation means the aortic valve leaks blood backward into the heart after every beat. The left ventricle slowly enlarges to handle the extra load. This process can continue for years without producing any noticeable symptoms.
Global Statistics and Epidemiology
Aortic regurgitation affects millions of people worldwide. Research published in the Journal of the American College of Cardiology estimates that moderate-to-severe aortic regurgitation affects around 0.5% of the general adult population—rising to approximately 2% after age 70.
According to the Global Burden of Disease study, valvular heart disease affects over 100 million people globally. Among these, aortic regurgitation is the second most common valvular condition after mitral regurgitation.
In countries like India, rheumatic heart disease — beginning with an untreated throat infection in childhood — remains one of the leading causes of aortic valve damage. AIIMS India and the Indian Council of Medical Research both highlight this as a significant public health concern, particularly in younger patients from rural communities.
In higher-income countries, the most common causes are bicuspid aortic valve—a congenital heart disease present from birth—and age-related valve degeneration.
Early Symptoms
In the early stages, most patients feel nothing unusual. When symptoms do begin to emerge, they tend to be easy to dismiss:
- Mild breathlessness during exercise — activities that never caused it before
- An awareness of the heartbeat, especially when lying on the left side at night
- Subtle fatigue after moderate activity
- Occasional palpitations — the heart thumping or fluttering noticeably
These are easy to attribute to stress, aging, or simply being less fit than before. That is why so many patients delay seeking medical advice.
Silent Symptoms — The Hidden Danger
This is the part that cardiologists worry about most.
The heart is an extraordinary organ. It adapts. It compensates. It keeps going quietly even when something is seriously wrong.
A patient can have significant valve leakage, measurable left ventricular enlargement, and early signs of weakening underneath the surface and still function essentially normally day to day.
Cardiologists call this the asymptomatic phase. It can last for years — sometimes a decade or more.
During this phase, the only reliable way to know what is happening inside the heart is through regular echocardiography. There is no feeling, no internal signal, no warning sign that tells a patient whether their heart is holding steady or quietly deteriorating.
This is exactly why a routine murmur picked up during a physical exam matters so much. It is often the only early clue that aortic regurgitation is present.
Summary:
During the silent phase, significant valve damage and left ventricular enlargement can develop with no symptoms whatsoever. Only regular echocardiography can track what is actually happening inside the heart during this period.
Emergency Symptoms
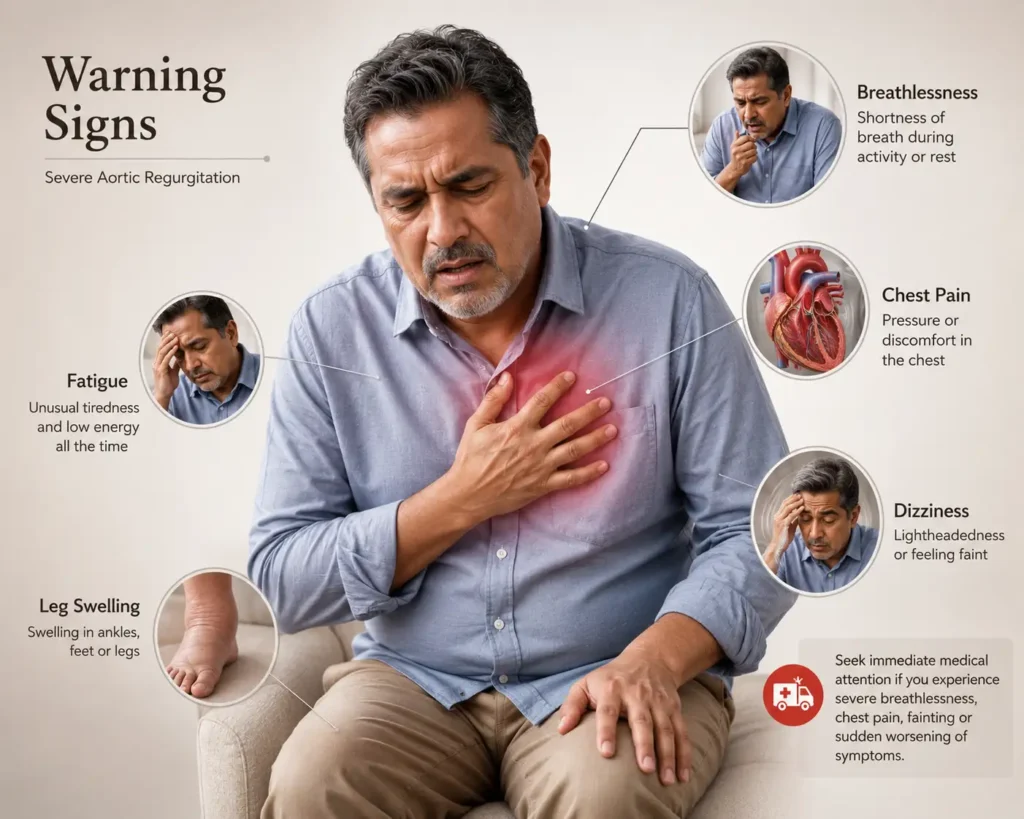
When the left ventricle finally reaches its limit, things can change rapidly. These symptoms require urgent medical attention:
- Significant breathlessness even at rest or when lying flat
- Waking at night unable to breathe properly
- Chest pain or tightness
- Severe fatigue with very little effort
- Swollen legs and ankles
- Dizziness or near-fainting episodes
Acute aortic regurgitation—caused by infections like endocarditis or aortic dissection—is a medical emergency. Symptoms appear suddenly and worsen fast. Call emergency services immediately if severe breathlessness, chest pain, and a rapid weak pulse develop together without warning.
Causes of Aortic Regurgitation
Bicuspid aortic valve —
a form of congenital heart disease where the valve develops with two leaflets instead of three. Present in 1–2% of the population, it is the most common cause in younger patients in higher-income countries.
Rheumatic heart disease —
caused by repeated untreated strep throat infections in childhood. It is still the leading cause of aortic regurgitation across South Asia, Sub-Saharan Africa, and parts of Latin America.
Infective endocarditis —
A bacterial infection of the valve causes rapid tissue destruction. A major cause of acute aortic regurgitation.
Aortic root dilation —
conditions like Marfan syndrome, chronic high blood pressure, and aortic aneurysm stretch the root of the aorta until the valve can no longer close properly.
Degenerative valve disease —
age-related calcification and stiffening. Increasingly common after age 65.
Risk Factors
- Age over 65
- Male sex
- History of rheumatic fever or repeated untreated throat infections
- Known bicuspid aortic valve
- Poorly controlled blood pressure
- Connective tissue disorders including Marfan syndrome
- Family history of aortic valve or aortic root disease
- History of intravenous drug use — a significant risk for endocarditis
- Autoimmune conditions including lupus and ankylosing spondylitis
Types and Severity Stages
Chronic aortic regurgitation develops gradually over months to years. The left ventricle slowly enlarges to handle the extra volume. Most patients remain without symptoms for a long time.
Acute aortic regurgitation develops suddenly. The heart has no time to adapt. Pulmonary edema and cardiovascular collapse can follow rapidly. This is always a surgical emergency.
Severity stages:
Stage | Findings | Symptoms | Recommended Action |
|---|---|---|---|
Mild | Small valve leak | Usually none | Echocardiography every 3–5 years |
Moderate | Moderate leak with mild LV enlargement | Mild or no symptoms | Echocardiography every 1–2 years |
Severe (Asymptomatic) | Large leak with significant LV enlargement | No symptoms yet | Echocardiography every 6–12 months |
Severe (Symptomatic) | Severe leak with LV dysfunction | Breathlessness, fatigue, chest discomfort | Surgery strongly recommended |
Pathophysiology Explained in Simple Words
With every heartbeat, the leaking valve sends blood back into the left ventricle. The ventricle stretches to accommodate it. For a while, the ejection fraction—the percentage of blood pumped out with each beat—stays normal. The patient feels fine.
But the stretched walls begin generating higher internal stress. To compensate, the heart builds extra muscle. The ventricle becomes both enlarged and thickened.
Over years, this sustained volume overload leads to myocardial fibrosis—permanent scarring of the heart muscle. Once significant fibrosis develops, surgery can relieve the valve problem but may not fully restore normal heart function.
As Dr. Valentin Fuster and the team behind Braunwald’s Heart Disease have emphasized for decades, the window for intervention before irreversible damage is the most critical decision point in managing aortic regurgitation.
This is why early surgery for aortic regurgitation is not aggressive or premature. It is protective.
Why Symptoms Can Be Misleading
Most patients diagnosed with aortic regurgitation ask the same question. “If I feel fine, how can anything be seriously wrong?”
It is a fair question. But the honest answer is this—the heart is designed to compensate. It adapts quietly. It stretches. It builds more muscle. It finds a way to keep going.
What the heart cannot do is tell you when that compensation is running out.
By the time breathlessness, fatigue, or chest discomfort appears, the left ventricle may already be significantly weakened. The symptoms arrive late — often after permanent changes have already taken root.
This is why waiting for symptoms is not a safe strategy in aortic regurgitation. It feels like wisdom. It can turn out to be the most costly decision.
Why Early Surgery for Aortic Regurgitation Matters
The 2021 ACC/AHA Guidelines for Valvular Heart Disease—the globally recognized clinical standard—recommend surgery for severe aortic regurgitation when:
- Symptoms develop
- The ejection fraction falls below 55%
- The left ventricular end-systolic diameter exceeds 50 mm
- The patient is already undergoing cardiac surgery for another reason
The critical point is that two of these four triggers — ejection fraction and ventricular size — can be reached while a patient still feels completely normal.
A landmark study by Dujardin and Enriquez-Sarano published in Circulation established that once symptoms appear in severe aortic regurgitation, mortality without surgery reaches approximately 10% per year. Patients who received timely early surgery for aortic regurgitation before ventricular function declined had dramatically better long-term survival.
Research from the Cleveland Clinic and Harvard Medical School has consistently reinforced this—the heart that is operated on before it fails recovers far better than the heart that waits.
Summary:
Early surgery for aortic regurgitation protects the heart before irreversible weakening and scarring develop. Waiting for symptoms often means waiting until permanent damage has already occurred. Timely surgery gives the heart its best chance to recover fully.
How Doctors Decide Surgery Timing
The decision is never taken lightly. It involves careful assessment of:
- Echocardiography measurements — ventricular size, ejection fraction, valve leak severity
- Cardiac MRI — now considered the most accurate tool for quantifying regurgitant volume and ventricular function, particularly when echocardiography results are borderline
- Exercise stress testing — to detect hidden limitation in patients who report feeling well
- Blood pressure control — uncontrolled high blood pressure accelerates both valve deterioration and aortic root dilation
- Rate of progression — how quickly the ventricle is enlarging between consecutive imaging studies
Dr. Stavros Drakos and colleagues have contributed important research showing that serial echocardiographic monitoring is not passive waiting. It is active tracking with defined action thresholds.
Diagnosis and Imaging Tests
Echocardiography and Cardiac MRI
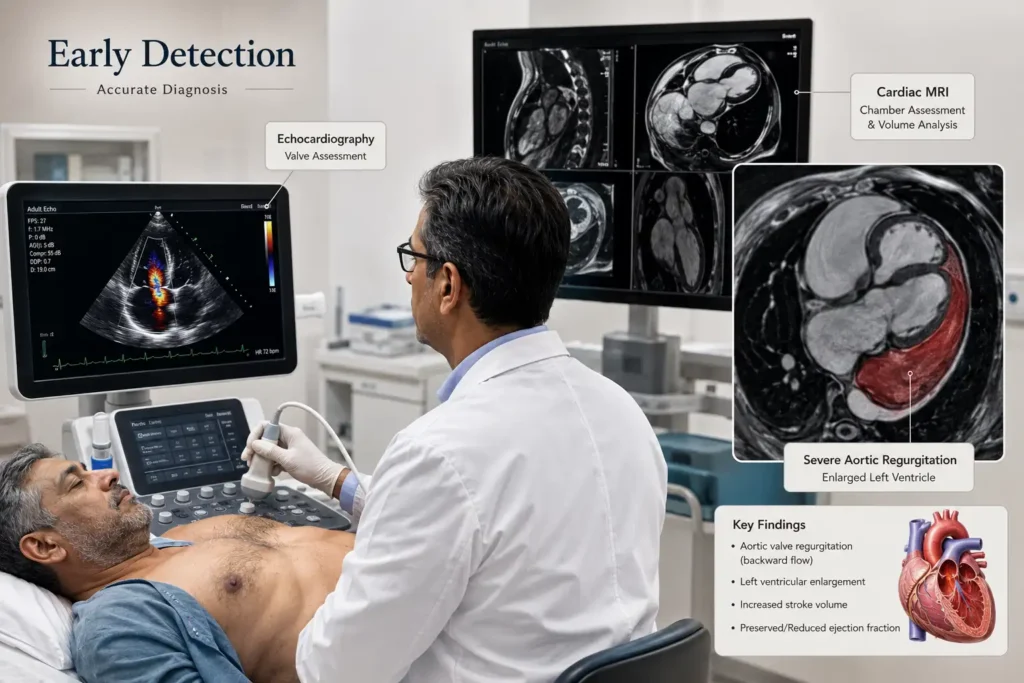
Echocardiography remains the cornerstone of diagnosis and monitoring. It measures the severity of valve leakage, left ventricular size, ejection fraction, and aortic root dimensions. It is safe, widely available, and can be repeated over time to track progression.
Cardiac MRI is increasingly used when echocardiography results are uncertain. It provides precise quantification of regurgitant volume and is particularly valuable in patients with borderline measurements where surgical timing decisions are being made.
Other investigations include:
- Chest X-ray — to assess heart size and detect pulmonary congestion
- ECG — to identify voltage changes suggesting ventricular enlargement
- CT angiography — used when aortic root dilation or aortic dissection is suspected
- Cardiac catheterization — reserved for selected cases when non-invasive imaging is insufficient
Treatment Options
Medications
No medication can close a leaking valve. But medications manage the consequences and reduce the rate of progression:
- ACE inhibitors or ARBs — lower blood pressure and reduce ventricular workload
- Beta-blockers — used carefully for heart rate and blood pressure management
- Diuretics — reduce fluid retention and breathlessness in patients developing early heart failure symptoms
- Antibiotic prophylaxis — recommended before certain dental procedures in patients with prior valve surgery or history of endocarditis
Valve Repair vs Valve Replacement
Aortic valve replacement is the definitive treatment. Options include:
Mechanical valve —
extremely durable, but requires lifelong anticoagulation with warfarin. Preferred in younger patients who can manage long-term medication.
Biological tissue valve —
No anticoagulation is needed, but it may require re-intervention after 15-20 years. Preferred in older patients.
Valve repair —
preserves the patient’s own valve tissue. Technically demanding and only suitable for specific anatomical cases, but it avoids prosthetic valve complications entirely when successful.
TAVR —
Transcatheter aortic valve replacement. Currently used mainly in high surgical-risk patients. Dedicated devices for aortic regurgitation are in active clinical trials.
What Happens If Surgery Is Delayed
Delaying early surgery for aortic regurgitation, when it is genuinely indicated, carries real consequences.
The left ventricle can reach a point from which full recovery is no longer possible. Myocardial fibrosis, permanent scarring, accumulates quietly. Once significant fibrosis is established, even a technically perfect valve replacement may not restore full ventricular function.
Untreated severe symptomatic aortic regurgitation carries a mortality of approximately 10% per year. Patients with heart failure symptoms have average survival under two years without intervention.
Beyond the heart itself, progressive cardiac dysfunction increases the risk of complications affecting other organ systems — including peripheral artery disease and kidney impairment, both of which worsen when cardiac output remains chronically reduced.
Conditions like heart attack heart failure, and STEMI and NSTEMI events become increasingly likely as ventricular function deteriorates. The comparison to normal heart rate — the simple, steady rhythm a healthy heart maintains — feels distant for patients who have reached this stage.
The tragedy is that this entire cascade is often avoidable. Early surgery for aortic regurgitation, timed correctly, protects the heart before the damage becomes irreversible.
Summary:
Once symptoms appear in severe aortic regurgitation, the prognosis without surgery worsens rapidly. Permanent scarring of the heart muscle, progressive heart failure, and rising mortality are the consequences of waiting too long for intervention.
Recovery After Valve Surgery
Most patients are genuinely surprised by how well they feel after surgery — especially those who had been quietly carrying significant ventricular strain without realizing it.

- Hospital stay: 5-7 days for uncomplicated open surgery
- Breastbone healing: 6-8 weeks
- Return to light activity: 2-4 weeks
- Return to driving: 4-6 weeks
- Return to office work: 4-6 weeks
- Full recovery: 3-6 months
Cardiac rehabilitation—supervised exercise beginning around 4-6 weeks post-surgery—significantly improves both physical recovery and emotional well-being. The Cleveland Clinic and Imperial College London both emphasize rehabilitation as an essential part of the post-surgical journey, not an optional extra.
Life Expectancy and Prognosis
Outcomes after aortic valve replacement are genuinely excellent when surgery is performed before irreversible ventricular deterioration occurs.
Ten-year survival after timely valve replacement exceeds 70-80% in major surgical series—approaching what would be expected for the general population of the same age group.
Mild aortic regurgitation managed with appropriate monitoring carries a normal life expectancy. Severe aortic regurgitation treated with early surgery before the ventricle fails—most patients return to near-normal life.
The single most important factor in long-term outcome is not the severity of the leak. It is whether ventricular function was preserved at the time of surgery.
Diet and Lifestyle Changes
Reduce sodium intake —
target below 1,500-2,000 mg daily. Excess sodium worsens fluid retention and raises blood pressure, both of which add further strain to an already overworked heart.
Increase potassium-rich foods.
bananas, spinach, sweet potato, and avocado help support blood pressure regulation naturally.
Omega-3 fatty acids —
from fatty fish like salmon, sardines, and mackerel — reduce inflammation and support cardiac function.
Avoid saturated fats, processed foods, excessive alcohol, and sugary drinks. These contribute to the same vascular risk factors—including blood pressure dysregulation—that accelerate valve and aortic root disease.
Exercise Recommendations
Mild to moderate aortic regurgitation: Regular moderate aerobic activity is safe and beneficial. Walking, swimming, and cycling are excellent choices. Aim for 150 minutes of moderate activity weekly.
Severe asymptomatic aortic regurgitation: Low to moderate aerobic activity is generally acceptable. Avoid competitive sports and heavy resistance training. Discuss your specific exercise program with your cardiologist.
Post-surgery: Supervised cardiac rehabilitation is the safest and most effective approach. Structured exercise after valve replacement accelerates physical and emotional recovery.
Prevention Tips
- Treat strep throat completely and promptly with antibiotics — this prevents rheumatic heart disease, one of the most common preventable causes of aortic valve damage globally
- Control blood pressure consistently — even modest reductions in systolic pressure reduce aortic root stress significantly
- Maintain excellent dental hygiene to reduce the risk of endocarditis
- If a first-degree relative has a bicuspid aortic valve — get echocardiography screening even without any symptoms
- Avoid intravenous drug use — a significant risk factor for endocarditis and acute valve destruction
When to See a Doctor
Schedule an appointment if you notice:
- New or worsening breathlessness during activities that were previously easy
- Unexplained fatigue or declining stamina
- Palpitations — the heart thumping, racing, or beating irregularly
- New swelling in the legs or ankles
- Any chest discomfort
- You have been told you have a heart murmur but have never had an echocardiogram
Emergency Warning Signs
Call emergency services immediately if you experience:
- Sudden severe breathlessness
- Chest pain at rest
- Dizziness, fainting, or near-fainting
- Cold and clammy skin with a rapid weak pulse
- Sudden extreme weakness or confusion
These may indicate acute aortic regurgitation, a heart attack, or decompensated heart failure—all of which are life-threatening emergencies requiring immediate care. Do not drive yourself to the hospital. Call for help immediately.
Latest Research and Expert Insights
Research continues to evolve how and when to intervene in aortic regurgitation.
Dedicated TAVR devices for aortic regurgitation—unlike aortic stenosis, where catheter-based valve replacement is now standard—present unique anatomical challenges. New dedicated devices are in clinical trials at major centers including Imperial College London and the University of Toronto.
Biomarkers for surgical timing — researchers are investigating whether BNP and NT-proBNP levels can identify asymptomatic patients approaching the critical threshold before echocardiographic changes become obvious.
AI-assisted echocardiography—Machine learning is being validated to improve consistency in measuring valve leakage across different imaging centers, reducing the variability that sometimes complicates surgical timing decisions.
Earlier intervention thresholds—emerging data from the Cleveland Clinic and other major centers suggest the current echocardiographic cutoffs for surgery may actually be too conservative. Studies suggest ventricular scarring may begin at lower thresholds than previously recognized.
Dr. Howard Eisen and Dr. Manjinder Singh Sandhu have both contributed to the growing body of evidence supporting earlier, proactive intervention in carefully selected asymptomatic patients with severe aortic regurgitation showing rapid ventricular progression. The principles outlined in Rapid Interpretation of EKGs and the broader framework of Braunwald’s Heart Disease continue to anchor clinical decision-making in this field.
Frequently Asked Questions
Can severe aortic regurgitation exist without symptoms?
Yes — and this is exactly what makes it dangerous. The heart compensates so effectively that patients can have severe valve leakage, significant left ventricular enlargement, and early ventricular dysfunction while feeling completely normal. This is why regular echocardiography is essential. Symptoms alone are not a reliable guide to how serious the condition has actually become.
Why do doctors recommend surgery before symptoms appear?
Because by the time symptoms develop, the left ventricle may already have reached a point where full recovery after surgery is no longer possible. Early surgery for aortic regurgitation — when the ventricle is still functioning well — gives the heart its best chance to recover completely. Waiting for symptoms often means waiting until permanent damage has already taken hold.
Can the heart recover after valve surgery?
Yes — and often remarkably well. When surgery is performed before irreversible ventricular scarring develops, the left ventricle can return close to normal size and function over several months following valve replacement. Many patients describe feeling genuinely better after recovery than in the years before symptoms appeared.
What happens if surgery is delayed too long?
Permanent scarring — myocardial fibrosis — develops in the heart muscle. Once significant fibrosis is present, even a successful valve replacement may not restore full heart function. This is the central reason why early surgery for aortic regurgitation matters so much. Surgery fixes the valve. But it cannot undo damage that has already become permanent.
Is exercise safe with aortic regurgitation?
For mild to moderate aortic regurgitation, regular moderate aerobic exercise is safe and beneficial. For severe aortic regurgitation, low- to moderate-activity is generally acceptable, but competitive sports and heavy resistance training should be avoided. Always discuss your specific exercise program with your cardiologist before making significant changes.
Can patients live normally after valve surgery?
Most patients return to full normal activity within three to six months after surgery. Driving, working, exercising, traveling—all become possible again. Many people describe life after successful valve replacement as genuinely better than the years they spent unknowingly adapting to a compromised heart.
Is valve replacement dangerous?
All surgery carries some risk. But aortic valve replacement is one of the most performed and most studied cardiac surgeries in the world. In experienced centers, operative mortality for elective valve replacement in patients with preserved ventricular function is below 2-3%. The risk of not operating when surgery is clearly indicated is far greater.
What is the survival rate after surgery?
Ten-year survival after timely aortic valve replacement exceeds 70-80% in major surgical series. Patients who undergo early surgery for aortic regurgitation before ventricular dysfunction develops have outcomes approaching the survival rates of the general population of the same age group.
Can young adults develop aortic regurgitation?
Yes. A bicuspid aortic valve—a congenital heart disease present from birth—is one of the most common causes of aortic regurgitation in younger adults. Rheumatic heart disease, caused by untreated throat infections in childhood, affects young people significantly across India and many other parts of the world. Young adults with known valve conditions need regular cardiac monitoring.
How often should echocardiography be repeated?
- Mild aortic regurgitation: every 3-5 years
- Moderate aortic regurgitation: every 1-2 years
- Severe asymptomatic aortic regurgitation: every 6-12 months with close clinical review
- Any change in symptoms: immediate reassessment regardless of scheduled interval
Conclusion
Aortic regurgitation is often silent — until the damage is already done.
Research consistently shows that the best outcomes belong to patients who act early, before symptoms appear.
Stay close to your cardiologist. Keep your echocardiogram appointments. Know your numbers.
A heart monitored carefully and treated at the right time has every chance for a strong and healthy future.
Medical Disclaimer
Aortic regurgitation is often silent — until the damage is already done.
Research consistently shows that the best outcomes belong to patients who act early, before symptoms appear.
Stay close to your cardiologist. Keep your echocardiogram appointments. Know your numbers.
A heart monitored carefully and treated at the right time has every chance for a strong and healthy future.
About the Author
Iraphan Khan, BSN | D.Pharm | CMLT, is a Healthcare SEO Strategist and Medical Content Writer at RealMedVision, creating clinically accurate content optimized for Google and AI search.
Medically Reviewed By
Dr Praveen Verma, MBBS, MD — Diagnostic & Pathology
Dr Himanshu Morya MBBS — Clinical Accuracy & Patient Safety
Kalpna Singh Shekhawat BSN NP — Patient Care & Practical Accuracy
References:
- American College of Cardiology (ACC) / American Heart Association (AHA) Guidelines for the Management of Valvular Heart Disease, 2021
- Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine
- Mayo Clinic Cardiology by Joseph G. Murphy
- Journal of the American College of Cardiology (JACC)
- Circulation Journal — Aortic Regurgitation Research Studies
- National Institutes of Health (NIH)
- Cleveland Clinic — Aortic Valve Disease Resources
- World Health Organization (WHO) — Rheumatic Heart Disease Data
- AIIMS India and Indian Council of Medical Research (ICMR) Publications
- Rapid Interpretation of EKGs by Dale Dubin